Hormonal support after embryo transfer. Endometrial support in the eco program
The main function of sexual secrets is to create favorable conditions for the fertilization of the egg and the normal course of pregnancy.
A woman preparing to become a mother monitors the indicators of hormones, their change. Especially for the rate of estradiol in IVF after embryo transfer.
In the first week after the transfer of embryos under the in vitro fertilization program, follicles begin to grow in the ovaries of a woman, so the body produces estradiol after embryo transfer. Thanks to this hormone, the endometrium is created inside the uterus.
In the middle of the cycle, after artificial insemination in large quantities, the woman's body begins to produce a substance that guarantees the normal course of pregnancy - progesterone.
Progesterone and estradiol after the transfer of embryos that the corpus luteum produces are necessary for the full development of the unborn baby.
For the upcoming pregnancy, the level of progesterone is very important, since this hormone creates favorable conditions for the attachment of embryos during implantation, as well as further nutrition of the unborn baby.
The amount of progesterone after embryo transfer and estradiol is determined directly on the day of transfer of the fertilized egg, and then after 7 days.
Estradiol and progesterone after embryo transfer
The level of the hormone estradiol is important in the process of bearing a fetus. If the concentration of this hormone is low, it can lead to miscarriage.
The level of progesterone is also important for the expectant mother. A blood test to determine the norm of hormones after IVF transfer is a standard test that is prescribed to a woman during in vitro fertilization.
If the indicators fall, then the obstetrician-gynecologist prescribes hormonal preparations to the woman.
The rate of hormones at certain intervals is different. The IVF protocol states that initially the level of estradiol is determined before embryo transfer, and then the dynamics of this indicator is controlled.
The hormone estradiol is produced partially by the adrenal glands and ovaries. It is important in the formation of the fetus, because it affects metabolic processes, is responsible for the formation of the skeletal system of the unborn baby.

In addition, the hormone promotes stretching of the tissues of the uterus, which is necessary for a growing fetus. Estradiol has an effect on the cardiovascular system of a woman, due to which blood flow to the fetus increases, and, accordingly, nutrition.
Table of norms of indicators
Progesterone after embryo transfer is produced in the corpus luteum for the first four months. And after twelve weeks, the maturation of the placenta, which is responsible for the production of this hormone, begins.
After IVF, the level of sexual secretions in the woman's bloodstream increases daily, which serves as a beacon of the pregnancy process.
What should be the progesterone after embryo transfer and what do the deviations mean? The normal value of this indicator ranges from 6.9 to 56.6 nmol / l.
But if the level of the hormone fell below normal, then the likelihood of a miscarriage is high. Then hormonal support with medications is urgently needed.
The rate of estradiol and progesterone after embryo transfer is determined by:
- on the day of IVF;
- three days after the procedure;
- one week after embryo transfer;
- in two weeks.
Also, the reproductologist may prescribe additional laboratory tests according to indications. In some cases, progesterone control is even prescribed after embryo transfer by day.
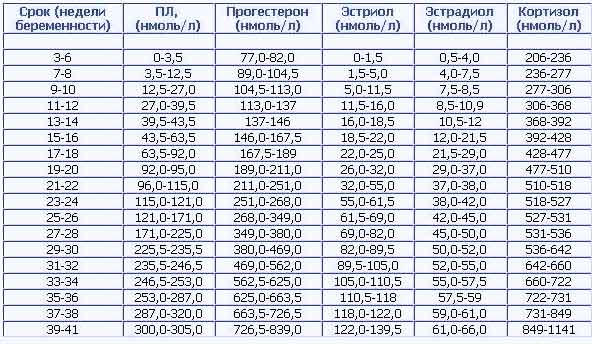
The table shows the norms of estradiol and progesterone during in vitro fertilization by week of pregnancy:
Progesterone and Estradiol levels by week of pregnancy
| weeks of pregnancy | Indicators of estradiol, nmol / l | Indicators of progesterone, nmol / l |
| 1–2 | 211–401 | 38–58 |
| 5–6 | 1061–1481 | 59–69 |
| 7–8 | 1381–1751 | 65–75 |
| 9–10 | 1651–2291 | 73–88 |
| 11–12 | 2281–3121 | 92–101 |
| 13–14 | 2761–4301 | 96–127 |
| 15–16 | 5021–6581 | 124–171 |
| 17–18 | 4561–7741 | 111–189 |
| 19–20 | 7441–9621 | 122–188 |
| 21–22 | 8261–11461 | 141–221 |
| 23–24 | 10570–13651 | 189–247 |
| 25–26 | 10891–14091 | 197–278 |
| 27–28 | 11631–14491 | 251–341 |
| 29–30 | 11121–16221 | 270–326 |
| 31–32 | 12171–15961 | 323–403 |
| 33–34 | 13931–18551 | 336–381 |
| 35–36 | 15321–21161 | 322–433 |
| 37–38 | 15081–22851 | 356–468 |
| 39–40 | 13541–26961 | 421–546 |
Low estradiol
During pregnancy, estradiol levels can be below normal for several main reasons:
- severe weight loss;
- significant physical activity;
- vegetarianism or lack of fats and carbohydrates in the body;
- bad habits, including smoking and drinking alcohol;
- hyperprolactinemia;
- dysfunction of the pituitary gland.

Heavy physical activity is the reason for no level of estradiol
In addition, estradiol, progesterone after the transfer of a fertilized egg can fall with the threat of abortion, with chronic diseases of the genitourinary system, as well as with the use of certain medications.
A decrease in the level of estradiol in the blood of a pregnant woman indicates that the placenta is in poor condition. In this case, the expectant mother is prescribed a special hormonal therapy:
- hormonal pills;
- injections;
- special patches.
In addition, the use of Proginov or Estrofem may be indicated.
If the hormonal background is disturbed in late pregnancy, this can cause the fetus to overbear (delayed labor activity). Then, to stimulate childbirth, the obstetrician-gynecologist may prescribe hormone therapy to the woman.
Low progesterone
During pregnancy, progesterone levels in the blood gradually increase, reaching maximum values in the third trimester. Since this hormone relaxes the muscles of the uterus, low progesterone after embryo transfer during in vitro fertilization is accompanied by severe pain and spotting.
If the above symptoms appear, the woman should immediately consult a doctor, otherwise a miscarriage may occur. And also a decrease in hormonal levels can signal that there is a delay in the development of the fetus.
The most common causes of low progesterone levels in pregnant women include:
- disorders associated with the development of the corpus luteum;
- strong physical activity;
- oxidative process occurring in the uterine cavity;
- delayed fetal development;
- insufficient functioning of the placenta.

Vegetarianism is the cause of low progesterone
In addition, the level of this hormone can be affected by the use of certain medications.
But an excess of progesterone in a pregnant woman may indicate the development of a pathological process in the body.
If the process of bearing a baby proceeds favorably, then in medical practice a reduced level of progesterone is observed very rarely.
If one of the symptoms listed above is detected, the patient who has undergone IVF should immediately contact the medical specialist who is observing her.
In no case should you try to increase the level of hormones on your own, because only the attending physician will be able to choose hormone therapy that will help to cope with the problem.
Conclusion
When conducting IVF, it is especially important to control the hormonal background of a woman. With artificial insemination, progesterone levels can be below normal, so many reproductologists recommend hormone therapy before and after embryo transfer.
But self-medication is categorically contraindicated, only a doctor can prescribe an effective treatment.
Do not worry, because most hormonal drugs are of natural origin and are completely safe for the body of a woman and her unborn baby.
Video: Hormonal examination. LH, FSH, progesterone
This article is devoted to the latest scientific achievements in the field of medicine and their implementation in IVF practice at the Nuriev Clinic.
Conditional abbreviations:
HCG - human chorionic gonadotropin - pregnancy hormone.
VT - corpus luteum
Question one.
What drugs to use to support the IVF program?
The corpus luteum of a woman produces two hormones: estradiol and progesterone. In general, the corpus luteum produces much more of them, but to simplify the explanations, we will assume that there are still two.
The main hormone is progesterone.
Historically, progesterone was used in injections, and injected intramuscularly into the soft spot 3 to 6 times a day. If anyone has had the experience of using "oil injections", he has a good idea of what happens to the fifth point after a couple of weeks of treatment! Therefore, when the French firmBesins proposed to insert progesterone into the vagina, there was a real breakthrough in improving the quality of life of a woman, no worse than the invention of pads or a washing machine. Women really did not appreciate it, and doctors had to be convinced for about ten years that the vaginal form was no less effective than the injectable one. But the fact remains: 600 mg of micronized progesterone (Utrozhestan) is equivalent to 6 injections of an oily solution per day.
A little later, Crinon, a gel in suppositories for vaginal use, was introduced to the market, similar, but more convenient - it can be inserted only once a day (Utrozhestan must be inserted at least twice a day, preferably three). One suppository of krynon is equivalent to 800 mg of utrogestan.
Despite the high price, Crinon is used in IVF programs at the Nureyev Clinic. There are at least two advantages of the drug:
the first - a single daily administration is more reliable, it is more difficult to forget / miss it. With Utrozhestan, such problems sometimes occur, which is sensitive for the IVF program.
the second - Kraynon leaks less, especially in summer, which is more comfortable. But there is no fundamental difference.
But it is with the drug Duphaston. The drug is synthetic, not progesterone, but its analogue. The safety of use during pregnancy has not been clearly established. Therefore, we do not use it.
For those who want to read more, here is a link to the doctors' discussion (note the dates):
** **
The second essential hormone is estradiol. It exists in two forms: tablets (proginova, estrofem) and gel for cutaneous application (divigel, estrogel).
Estradiol, being introduced into the body of a woman in a sufficient dose (2-3 tablets per day), in combination with progesterone, can keep the endometrium in a stable state for quite a long time. It leads tofalse the feeling that high doses of two drugs - estrogen and progesterone - can prevent miscarriage or improve IVF outcomes. Unfortunately, no high doses of drugs can make a good embryo out of a bad one (on the contrary, they can!). Therefore, there are standard doses of standard hormones for women of the homo sapiens species, these doses are: progesterone 600 mg per day, estradiol 2 mg (tablet) twice a day. Everything else is redundant.
"How so?!" - every second of my patients asks me - “Can I add a dose, this is important for me, let my chances of getting pregnant be higher! You can’t spoil porridge with butter!” Spoil it. Excessive doses of hormones (both) in animal studies have shown effect on the fetus. No such tests have been conducted on women.
Therefore, any deviation from the standard is not welcome. An overdose, like an underdose, is undesirable, because it deviates us from the optimum, from the dose recommended for our species. So we tend to prescribe standard doses in standard situations, that is, we act according to a template. So standard that instruction on the use of drugs in this group is assigned to the duties of a nurse. And we are not ashamed of this pattern. The doctor has a place to apply his creative abilities. Anywhere but in support of the endometrium.
Question two. When to start and when to end support?
When to start. Science says that if you start supporting the endometrium on the day of follicle puncture, or the next day, or every other day, or on the third day, we get maximum results. If earlier or later, the results will be worse. The sooner, or the later, the worse.
when to finish? More difficult question. When I came to IVF, the typical support time was up to 12 weeks of pregnancy. Then the bar was lowered to seven weeks, then to 6 weeks.
Today it is believed that the withdrawal of all support drugs on the day when hCG is positive does not lead to termination of pregnancy. That is, you either have a pregnancy or you don't. And if hCG is positive (more than 50 units), then the drugs can be safely canceled.
Attention! All of the above applies only to the standard IVF protocol! Cryoprotocols, protocols with a donor egg or with a surrogate mother have some peculiarities - support goes on at least up to seven weeks of pregnancy! If you are not sure, be sure to check appointments/cancellations with the ART nurse or doctor.
And so, we start support on the third day after the puncture, we end on the day of the hCG test. Deviations from these rules are not welcome, since the frequency of progressive pregnancies does not increase from this.
But the price of the protocol and the side effects of drugs increase. What are the effects?
Obvious effects are: bloating, constipation, tissue swelling due to fluid retention, drowsiness and inhibition of reactions.
And not obvious effects: the doomed pregnancy will still be interrupted, but at a later date, causing significant damage to the woman's health. Over 80% of aborted pregnancies had gross violations of the chromosomal set of the embryo. That is, they could not be saved.
Therefore, support can be canceled earlier than it was accepted. Moreover, support SHOULD be canceled as early as possible.
Question three.
What to do if bloody spotting begins?
Nothing. Most often, spotting begins four days before the hCG test. This happens because its own, native corpus luteum has exhausted its resource and began to produce less progesterone and estradiol. If the embryo is implanted and begins to produce hCG, then it stimulates the corpus luteum and does not allow it to relax.
Bloody discharge before the hCG test is the first sign of a lack of implantation, and hence pregnancy.
If the discharge is scarce, it is not worth canceling the drugs. There are chances to keep the pregnancy, since only the lower layers of the endometrium have exfoliated, closer to the cervix (the embryo is transferred closer to the bottom of the uterus). If a full-fledged menstruation has come, there is no chance - you need to cancel support without specifying hCG.
Of course, it is psychologically very difficult to come to terms with the fact that the IVF protocol ended in failure. Too much effort has been put in. Of course, the intervention of large doses of drugs (estrogens, for example) can stop the bleeding that has begun. But do not keep the pregnancy. Because a bad embryo causes bleeding. And not vice versa.
Is it possible and necessary to call a doctor if you start bleeding? Of course! It is possible and necessary. In this case, as a rule, the doctor gives his mobile number at the beginning of treatment. However, we ran into a problem: the doctor has more than 100 a day! incoming calls to the mobile, most of them occur during the hours of the reception of other patients or during operating hours. The well-known anecdote about the gynecologist “two more times around the school” was really in my practice :-). Let's add here the dream of a doctor and a little personal life - it can be difficult to get through on the phone. As a compromise, we have introduced an emergency telephone, which is issued during procedures in the Clean Zone, and is always on duty with a nurse. She will either connect with the doctor, or replace the "native" doctor with a "foreign", but still competent, if her doctor suddenly cannot answer the call. Although we try not to leave “ours” in trouble. Especially after IVF. Especially when bleeding.
Question four.
What hormones should be monitored?
None. Because there are no rules. No hormone levels are a reason to change the current doses.
Why?
Because progesterone preparations, introduced vaginally, create high concentrations in the uterus and endometrium. And it's difficult to measure hormones there.
If the concentration of progesterone in the uterus is much higher than in the peripheral blood, then why measure progesterone in the blood? Then, that we can’t measure anywhere else :-)))
The study of the level of progesterone in the blood is a useless transfer of money, since no conclusions, no forecasts can be drawn based on the level of progesterone in the blood, and even more so, prescriptions cannot be adjusted. Everything about progesterone.
Estradiol. This hormone, even in small doses, can hold the endometrium. The sensitivity of women's tissues to this hormone is different and therefore the rate of estradiol is very blurred, it is also variable. Therefore, as with progesterone, a laboratory-determined level of estradiol is not a rationale for dose adjustment.
So why measure estradiol before and after embryo transfer? To determine the risk of developing ovarian hyperstimulation syndrome. But that's a completely different story. And a topic for another article.
Question five.
What else improves outcomes? Aspirin, clexane, fraxeparin, vitamin E, leeches? Anything else?
Nothing. None of the drugs registered in the world has shown any significant effect in increasing the frequency of pregnancy. Tales about "thick blood" were invented by pharmaceutical companies that produce "drugs against thick blood." These misconceptions, as well as stories about the miraculous salvation of an ECO pregnancy, are supported artificially, because the stars are burning because someone needs it.
On my own behalf, I note that a reproductive specialist feels a slight offense when he hears that any woman who, in self-medication, used potent drugs during the IVF protocol and got pregnant, glorifies this drug, advised him to a neighbor and providence. A slight insult, because a woman becomes pregnant from the fact and only from the fact that she had embryos transferred and a gigantic preparatory work was done before that.
Question six.
Sex life, bed rest, hospital, diet.
sex life does not increase or decrease the effectiveness of IVF. Live in health!
In doing so, remember the following:
condoms are very toxic because they contain spermicides - substances that kill all living things. Do not use them during an IVF program.
ovarian cysts formed during stimulation/puncture can be mechanically traumatized, causing pain (at least) and even bleeding. Be careful! If you can, of course :-))
Bed rest does not improve outcomes. Live as you wish! With the exception of sports activities. IVF for step aerobics or judo not best time(remember ovarian cysts!)
Hospital treatment , contrary to popular belief, does not improve, but rather worsens outcomes. Statistically proven. On a large sample. But why so - no one knows. Think for yourself. I have different thoughts about this, but I will be careful not to express them. I really don't like hospitalizing women to keep their pregnancy going. early dates'cause I'm losing control of my appointments. However, going to the hospital if you have problems, or not going to bed is your choice.
Diet . Heavy food - kebabs, dumplings, fried mushrooms and other tasty, but unhealthy foods, can be poorly accepted by the intestines, which already "tolerate" an excess of steroid hormones. So it's better not to experiment. In addition, weight is gained against the background of hormones much faster. I note that not only because of hormones, but also because of excess food and at the same time a decrease in motor activity after embryo transfer.
But there are no restrictions!
Question seven
(Which I never get asked, but in vain!). Are all medications given as support safe for me and my baby?
The answer is negative. The safety of estradiol for the health of an unborn child is unclear. Synthetic estrogens (the notorious des - diethylstilbestrol) showed a teratogenic effect on the female child and were banned from use during pregnancy. Modern preparations of estradiol, in principle, differ in structure from des, and "should not have" a teratogenic effect. Should not. Should not. Shouldn't or shouldn't? Science does not know this. Therefore, it is better not to use estradiol preparations after embryo transfer without need. What is considered a need? Read the next question.
Question eight. How does support depend on the type of IVF protocol?
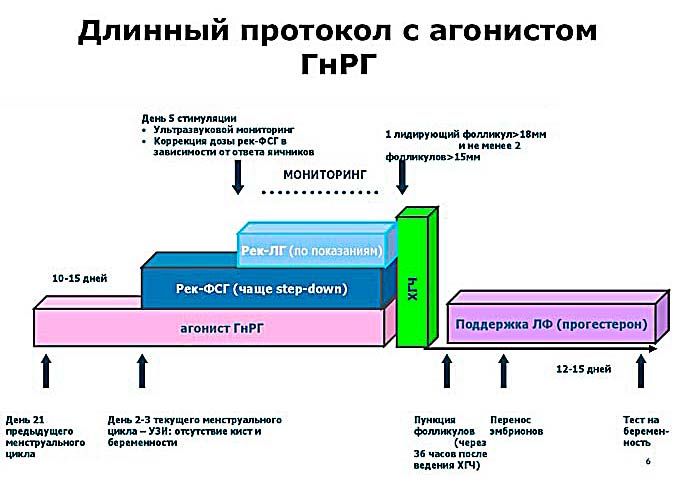
It depends very much. All of the above about estradiol and progesterone was said about the standard long protocol. The long protocol has historically been the first reliable treatment protocol with good results. In the long protocol, native hormones were suppressed the most and therefore good (great!) endometrial support was required.
Currently, the short protocol (we call it the antagonist protocol) is the most commonly used. And (good news!) for the protocol with antagonists, the use of estrogen in support is not mandatory. Quite the contrary: women who took and did not take estrogens had the same chance of becoming pregnant and enduring pregnancy. This is one of the good reasons why the long protocol is being heavily phased out of clinical practice by the antagonist protocol.
Question nine.
In what cases are hCG preparations used?
I almost forgot. Chorionic gonadotropin human, (pregnil, ovitrel) stimulates the corpus luteum of the ovaries and, therefore, is used to stimulate the endometrium. However, the probability of getting hyperstimulation syndrome on it is an order of magnitude greater, and the increase in pregnancies is insignificant. Therefore, we use these drugs if no more than five follicles have grown in the ovaries during stimulation (for both ovaries).
Question ten. What else do I need to know?
Advice for the future: this is a very good question, ask your doctors more often!
Answer:
The quality of drugs used for support is subjected to a thorough statistical analysis by the staff of the ART department. If a series of drugs is of poor quality (this is terrible, but it happens!), they (these drugs) are withdrawn from circulation as soon as possible. Therefore, the medicine that we give you almost always works without failure. Until you took him out of the clinic. If we control injectable drugs at all stages, up to the injection, then with drugs for support, everything is the other way around. Most of the time it is used and controlled by you. Room temperature in summer is often above 25 degrees above zero, which is critical for krynon, utrozhestan and proginova. Don't forget about it.
Perhaps, numerous myths about weak support appeared not least due to the fact that we have hot summers and cold winters?
Conclusion.
Often, in medicine, the approach of redundant prescriptions is used.
Money? Doesn't matter!
Risks? We don't know!
Side effects? Let's endure!
If it were only about these issues, it would probably not be worth devoting so much time to this topic. However, excessive attention to issues related to the support of the endometrium by yellow mist obscures real problem IVF: Most failures are not due to poor endometrial preparation and support, but to the quality of the embryo.
- - what proportion of good embryos did I have in the current protocol?
- - was the development of my embryos optimal for my age group?
- Could the stimulation have been better?
- - what could be done to increase the number of high-quality embryos for the next protocol, if pregnancy does not work out in this one?
That's probably all for now on this topic. See you on transfers!
And do not try to take hormonal drugs uncontrollably!
This article was written not for self-treatment, but for self-education!
The replanting of a fertilized egg to a woman does not mean that they did everything they could. From this moment on, it is necessary to regularly monitor the state of the fetus, the pelvic organs of a woman in order to prevent or stop undesirable situations that arise in time. In other words, conducting certain tests after embryo transfer can increase the chances of successful implantation, the normal course of pregnancy and the identification of possible fetal pathologies. Important! Only a specialist can give an adequate interpretation of research.
Hormones
Many patients independently, even if doctors do not prescribe it, take tests on the day of embryo transfer, and not only after replanting. It is better to do this in order to track the further "behavior" of indicators. So to say - the starting point will be the day of the transfer, then you need to watch the indicators grow or not, how they grow.
To reduce an overestimated or increase an underestimated result is a consequence of taking hormones during the period of preparation for IVF and certain manipulations (puncture, embryo transfer) or a real threat of protocol failure. In the first case, the indicators improve after retaking the tests in a day or two, in the second case, support may need to be adjusted after the transfer.
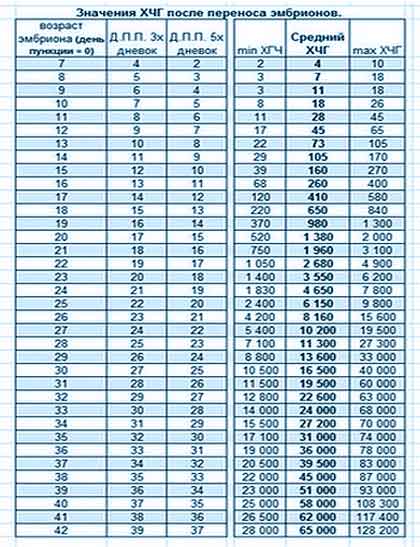
What hormones are given after embryo transfer? Starting from the first day, from the day of replanting, and then on days 3-5, 7-8 and 14, you can monitor the level of estradiol and progesterone. Estradiol and progesterone have an impact on successful implantation, normal development and gestation. On the 14th day, a comprehensive examination is done - more hCG is added to the indicated analysis. The level of the hCG hormone determines whether pregnancy has occurred or not.
What tests should be done after embryo transfer? In addition to hormones, sometimes you have to monitor the following tests:
- D-dimer;
- coagulogram;
- hemostasis;
- fibrinogen level.
All these indicators are important for the detection of pathologies of blood clotting. More often, only D-dimer is prescribed. If there were problems with coagulability and coagulants were prescribed before infusion, then the rest can be monitored. Sometimes it is difficult to determine the presence of a problem by one of them. An experienced hematologist evaluates the performance of all tests before voicing a diagnosis.
Dynamics
Before taking any tests after replanting on your own or as directed by a doctor, you must understand that the boundary norms for IVF will differ from the usual ones. The stimulation of the ovaries, the preparation of the woman's body for the adoption and bearing of the fetus includes a huge amount of hormones and other drugs.
Therefore, it is not so much the quantitative value of certain indicators that is important, but the actual dynamics of hormones after embryo transfer, as explained above.
Do I need to monitor hormones after embryo transfer? Sometimes doctors do not prescribe absolutely no tests, patients give up after two weeks from the moment of replanting only hCG level, only further ultrasound, screenings. It is necessary to understand that the amount of estradiol and progesterone is significant in the uterus, the concentration of these indicators in the blood does not always correspond to the real state of affairs. There (in the uterus) they have not yet learned how to measure them. And no one canceled the amount of drugs received in preparation for IVF, which also distorts the overall picture.
For example, in the results obtained, it is clear that hormones are growing - women are happy. Or vice versa, the result is less than the minimum allowable value - panic, and excessive tearfulness after embryo transfer already interferes with adequate perception of information.
Most physicians use hormonal monitoring to detect and control ovarian hyperstimulation syndrome, which may occur after embryo transfer.
It is logical that if the specialist has appointed - you need to take it, if not - either trust the doctor, or do not panic if the results turn out to be incomprehensible.
But, the fact remains that in a successful protocol, hormones after embryo transfer should ideally gradually increase by day. For this purpose, hormonal support is prescribed in the form of vaginal suppositories, sometimes up to 6-7 weeks of pregnancy.
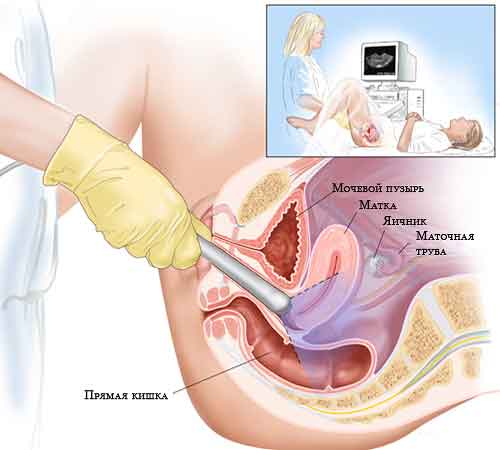
ultrasound
Another important procedure in the IVF protocol is ultrasound. Ultrasound examination can be performed transvaginally and transabdominally. The first option means that a special sensor will be inserted into the vagina, the second is the usual way, the sensor will scan through the front wall of the abdomen. The method is determined by the doctor, both methods are safe for the patient and the fetus.
Do they do ultrasound before embryo transfer? Of course, they do - before replanting, it is necessary to assess the thickness of the endometrium, the condition of the ovaries, and find out if there are any factors that contribute to the cancellation of the procedure. It may happen that the very process of implantation of the embryos will be carried out in parallel with the ultrasound examination to help the specialist.
![]()
On what day after the embryo transfer is the fertilized egg visible? It happens that an ultrasound scan of a patient needs to be performed ahead of schedule according to the protocol - monitoring of the state of OHSS is required, there are serious complaints of the client about pain, etc. During such examinations, it is possible to notice a fetal egg. On average, it can be caught at 15 DPO. But this is rare. The size of such a fetal egg is very small. Therefore, in all IV protocols, the first ultrasound is done to confirm pregnancy on day 21.
Ultrasound diagnostics is an obligatory component of the so-called "prenatal screening". This is a series of examinations that help determine the risks of giving birth to a child with severe pathologies. Ultrasound screening after IVF makes sense in combination with a biochemical (blood test for special markers of various genetic diseases).
Screening of the 1st trimester after IVF is optimally carried out at 11-13 weeks of pregnancy. It is customary to carry out an ultrasound scan first, during which the anatomical development of the fetus is established, the presence of anomalies is determined, and the size corresponds to the norms. For three days, and preferably on the same day, conduct a biochemical screening. It is important to remember that biochemical tests alone are not a diagnosis. In general, the whole procedure is not much different from screening during a normal pregnancy.
From the moment when the hCG test established pregnancy, and the first ultrasound confirmed it, a woman after IVF becomes "the most ordinary pregnant woman", like a woman with a natural conception. The same risks, problems, experiences. They are the same for all expectant mothers.
The ability of the female body to conceive is determined by the production of a special hormone by the corpus luteum. Progesterone is most important in IVF - its indicators predetermine the success of fertilization. Therefore, it is so important to keep it normal with medications.
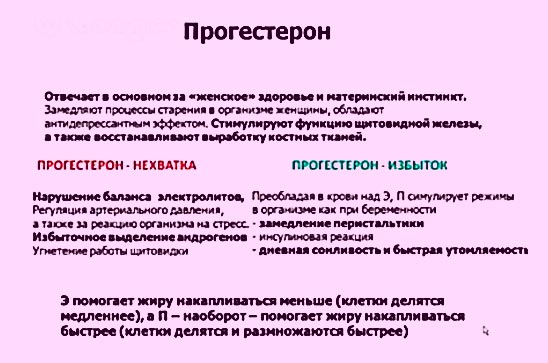
"Duties" of the hormone
Under natural conditions, conception occurs if female body managed to prepare for ovulation. Yellow bodies begin active synthesis of the “pregnancy hormone” weeks 2 before the intended fertilization. If there is enough progesterone, the egg will fuse with the sperm. Otherwise, by the end of the cycle, the yellow bodies die, and the woman begins menstruation.
The main function of progesterone is to prepare the female body for reproduction. The hormone tries to create all the necessary conditions for this.
What does progesterone do:
- establishes the menstrual cycle, which provides normal conditions for conception;
- helps to reduce the contractile movements of the uterine muscles. This allows the embryo to be well fixed on the wall of the uterus;
- helps to maintain pregnancy throughout its duration, excluding the possibility of spontaneous abortion;
- promotes the restructuring of the glands for the production of milk by the time of childbirth.
If the female body is not able to independently produce the required amount of the hormone, the patient is prescribed medications that make up for the deficiency. But if this does not help to conceive naturally, the woman is sent for in vitro fertilization, where this hormone is actively used.
Planning for conception
Having planned to become a mother with the help of artificial insemination, a woman tunes in to the fact that progesterone before IVF will increase to the desired level with medications. Progesterone falls before menstruation, while its active synthesis occurs in the 2nd phase of the cycle.
Therefore, first they wait for regular allocations, and they start counting from them. On the 16-17th day, they begin to give the patient drugs that compensate for the deficiency of the hormone in the body. They have a stimulating effect on the corpus luteum, and also help the endometrium grow to the desired level.
Before the end of the cycle, the patient takes hCG tests. If progesterone is elevated during IVF, most likely the pregnancy has taken place. Due to the risk of miscarriage in the initial stages, continue to take progesterone in the first days of pregnancy up to 12 weeks (and more - if necessary). Further, the formed placenta performs the function of maintaining this hormone.
The use of hormonal drugs continues until the 26th day of the cycle. Embryo replanting is carried out on the 3rd day from the start of hormone therapy, and cryoblasts - on the 5th day.
Is it possible to do IVF if progesterone is low? After undergoing hormonal stimulation, a woman takes tests immediately before the transfer. If it turns out that the progesterone level is low for fertilization, the IVF protocol is transferred to the next cycle. During this period, a woman should be additionally examined to understand the reason.
Period after planting
Not everything goes smoothly with the hormonal background after cryotransfer. Therefore, monitoring includes monitoring the condition of the patient who has undergone IVF in the first weeks after the protocol. Progesterone after the transfer is an important indicator not only of successful fertilization, but also of the general condition of the woman.
The rate of progesterone after replanting embryos is not always ideal. In half of the cases, there are deviations up or down. The patient can feel such conditions even physically - her chest hurts a lot, her stomach is significantly swollen and her mood changes for no reason.
Progesterone is especially important when smearing after IVF. These are vaginal discharges, and they may be minor, but bleeding is also sometimes observed.
To understand that this is a normal phenomenon, and not a threat of miscarriage, it is required to observe the hormonal level from the day of replanting for 2 weeks (and, according to some indications, even more).
How to donate blood for progesterone? It is advisable to take progesterone tests after IVF every 2 days in order to switch to hormonal support in time. Before taking blood, a woman should prepare - stop eating 8-10 hours in advance. Therefore, it is most convenient to take progesterone on an empty stomach, that is, in the morning after sleep.
The delivery of progesterone consistently during the first days after IVF will help to consider the trend of either a decline in the hormone or its rise, as well as identify deviations from the norm.
Hormonal standards
To understand what progesterone should be normal in the first days after embryo transfer, you should consider the table below. Progesterone increases every week, and by the time of delivery it will reach about 500 nmol / l. The table contains indicative data, since in different laboratories the indicators may vary slightly.
Table - The norm of progesterone during IVF by weeks
| Pregnancy period, weeks | Progesterone, nmol\l |
| 1-2 | 38 – 58 |
| 5-6 | 59 – 69 |
| 7-8 | 65 – 75 |
| 9-10 | 73 – 88 |
| 11-12 | 92 – 100 |
| 13-14 | 96 – 127 |
| 15-16 | 124 - 170 |
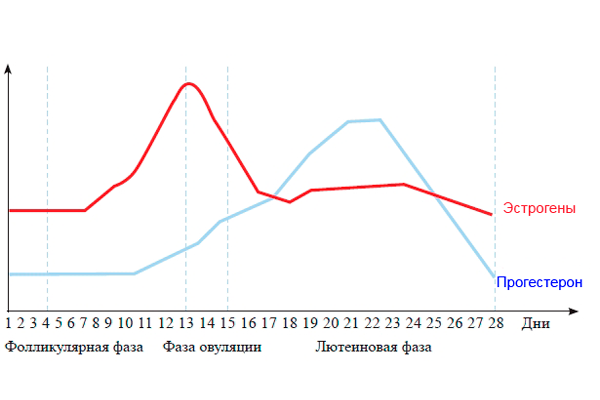
If you look at the level of the hormone in the blood at the end menstrual cycle, then it will be equal to 0 nmol / l. As soon as the ovaries enter the follicular phase, signs of progesterone begin to appear in the blood, the average value of which is 3 nmol / l. In the ovular phase, it already becomes at least 5 nmol / l.
Continuing to increase the amount of the hormone, the body enters the luteal phase, by the beginning of which the minimum indicator is more than 7 nmol / l. As soon as the embryo has entered the body, the level of progesterone begins to increase significantly - this is how nature takes care of the bearing of the fetus.
Deviation from the norm
As mentioned above, the hormonal background after IVF can deviate from the norm in both directions. If these deviations are too different from those necessary for the normal development of pregnancy, specific regulatory measures should be taken. But first you have to determine the reasons for the change in the background.
High progesterone:
- a sufficiently high jump in the level of the hormone may indicate abnormalities in the development of the placenta or the formation of a cyst on the corpus luteum;
- a deviation from the norm upwards may suggest the development of amenorrhea.
Low progesterone:
- if progesterone fell after replanting, the function of the corpus luteum may have been impaired;
- chronic inflammation of the ovaries can affect the indicator;
- when progesterone fell at 5-6 weeks of gestation, we can talk about the threat of miscarriage;
- a decrease in the level at subsequent dates is a reason to pay attention to the intrauterine development of the fetus (perhaps it is delayed).
An increase in progesterone on the day of the trigger will indicate an embryo transfer. The stable dynamics of the increase in the indicator in the following weeks is most likely a sign of pregnancy. In recent days, a low "pregnancy hormone" may suggest that a woman is walking.
Any deviation from the norm of the hormonal level can predict a brewing uterine bleeding. In any case, in order to maintain the pregnancy, you will have to resort to medical supportive drugs.
Hormonal Support
It is precisely the low hormonal indicator that poses a particular threat to abortion. To raise it, progesterone drugs are prescribed, which most often come in injections. Oily solution of transparent color "Urozhestan" is sold in ampoules of 1 ml of various concentrations (1% and 2.5%). They inject progesterone during IVF to reduce the risk of spontaneous abortion and strengthen the placenta.
How to give progesterone injections? To begin with, it should be clarified that the ampoules should be stored in the refrigerator. Before making an injection, the drug should be heated in warm water to body temperature. This will also allow the oily composition to be made more liquid so that it is easier to inject subcutaneously (in the shoulder, abdomen or buttock).


You should not get involved in hormonal drugs, since progesterone thickens the blood, which is not always a positive indicator and can lead to an increase in blood pressure. There are other consequences of the use of the described drugs.
Side effects:
- the drug can provoke vaginal bleeding in the first weeks after IVF, which is not always an indicator of an unsuccessful protocol;
- jaundice may develop due to cholestasis;
- drugs taken orally can cause dizziness with severe pain, as well as cause drowsiness;
- allergic manifestations in the form of rashes and itching of the skin are possible.
Before prescribing such medications, the woman will be informed of the consequences and side effects so that the described manifestations do not cause her to panic.
Progesterone is so important for bearing a fetus that a woman who dreams of becoming a mother will have to resort to hormone therapy to maintain the required level that promotes fertilization, as well as further development future baby. Preparations containing the “pregnancy hormone” become in most cases the basis for IVF protocols. They also help maintain the function of the corpus luteum in the following weeks of pregnancy, helping a woman give birth to a full-term and completely healthy baby.
Most women are prescribed medication support for IVF after embryo transfer. It depends on it how successfully the protocol ends. Several types of drugs are used.
A woman's health status, age, and the presence of unsuccessful previous protocols affect which drugs are prescribed after embryo transfer. IVF allows previously infertile couples to have a baby, but you must follow all the conditions of the protocol.
One of them is drug support for IVF after embryo transfer. If the doctor has not prescribed any drugs, you should clarify this point with him yourself. Since the preparations after embryo transfer help to preserve the pregnancy, which was so difficult for future parents.
Medications for support after embryo transfer
The range of drugs used in in vitro fertilization is very diverse.
It includes:
- vitamins;
- hormones;
- substances that prevent excessive blood clotting.
Post-transfer support drugs are needed to maintain the pregnancy and its normal course. Therefore, their appointment is very important.
The preparations after the transfer include an extensive list of vitamins. The most commonly prescribed complexes for pregnant women.
These include:
- Vitrum;
- Femibion;
- Elevit Pronatal.
The doctor may prescribe a vitamin complex himself, but sometimes leaves the choice up to future mother. All drugs are similar in composition and action, so there is no significant difference between them.
![]()
Important! When choosing a vitamin complex, it is worth considering the range of pharmacies closest to the place of residence, so that there is always the opportunity to buy exactly the remedy that was taken earlier. Changing the medicine during pregnancy is highly discouraged, especially if there is no allergic reaction or side effects to the prescribed drug.
Post-Embryo Transfer Support for IVF involves taking folic acid. She is prescribed in the same amount as all pregnant women.
The advantages of this acid are that it:
- prevents pathology of the neural tube of the fetus;
- helps the development of all systems of organs and tissues;
- prevents spontaneous abortion.
Folic acid can be taken alone or as part of complexes, if the amount corresponds to the prescribed dosage.

And also to support drugs after embryo transfer is magnesium, which has the following properties:
- helps reduce anxiety
- calm the nervous system;
- prevents the appearance of uterine tone.
It is prescribed in the form of preparations "Magne B6" or "Magnelis". These tablets, after embryo transfer, relax the woman's nervous system and prevent dangerous contractions of the uterine muscles that can provoke the rejection of fertilized eggs.

progesterone to maintain pregnancy
Hormonal drugs allow the embryo to gain a stronger foothold in the uterus, as well as to rebuild the body for a state of pregnancy. Progesterone has this effect.
Injections after embryo transfer with this drug are a fairly common phenomenon. But more often Progesterone is used in two forms:
- a gel that is inserted into the vagina (Krynon);
- capsules or suppositories used intravaginally (Utrozhestan).
The choice of dosage form is carried out by a gynecologist depending on the indications and purpose of treatment, as well as the patient's condition. Most often, candles are prescribed because of the ease of use.
Progesterone has several main properties:
- changes the structure of the endometrium, which facilitates the attachment of the embryo to the wall of the uterus;
- reduces the contractile activity of the uterine myometrium, allowing you to tightly close the cervical canal, reducing the risk of spontaneous miscarriage at the beginning of pregnancy.
Progesterone support after IVF is a common method of maintaining a long-awaited pregnancy. The drug is canceled gradually from 8 to 20 weeks.

The duration of admission is determined by the reproductive physician medical center performing in vitro fertilization. It is calculated based on the main indicators:
- the patient's history;
- type of IVF protocol;
- age;
- hormonal background of a woman;
- the presence or absence of artificial insemination prior to this experience and their results.
If you experience a severe allergic reaction or other side effects to drugs that support the luteal phase, you need to consult a specialist.
The doctor will select an adequate replacement medication. The drug should be discontinued gradually, reducing the dosage. Abrupt cancellation or skipping a dose is unacceptable, as this threatens the safety of the pregnancy.
Duphaston after transfer
This drug is also an analogue of human progesterone. Duphaston after embryo transfer helps to maintain pregnancy, ensure a successful course. The use of this drug is considered normal for in vitro fertilization protocols. Progesterone increases the chances of successfully implanting an egg in the endometrium of the uterus.
Dufaston belongs to the group of retroprogesterones. These drugs, used as luteal phase support in in vitro fertilization, have a strong progestogenic but low androgenic effect.
This gives them a number of advantages:
- lack of feminization of a male child;
- lack of masculinization of the organs of the reproductive system in a female child;
- does not affect the liver;
- does not affect blood clotting;
- does not cause rashes, hirsutism, change in voice towards the male;
- does not affect metabolic processes (does not change the concentration of blood glucose, as well as its lipid spectrum);
- no effect on the pituitary-ovarian system;
- does not cause adrenal atrophy.
Due to the presence of these properties, doctors actively prescribe Duphaston after transfer during artificial insemination. It is a dydrogesterone with a methyl group at position 10 in human progesterone).

This altered molecular structure allows Duphaston to be more easily absorbed during ingestion. The use of the drug in a dosage of 20 to 30 mg stimulates the secretion phase in the endometrium. Thus, dydrogesterone supports pregnancy.
The use of the drug begins from the moment of embryo transfer at a dosage of 30 to 60 mg per day. Reception continues until the 12th week of pregnancy. If there is a threat, treatment is extended up to 20 weeks.
Dufaston is absolutely safe for the fetus. The absence of a teratogenic effect has been confirmed by a mass of studies, so the drug is widely used as a support for artificial insemination.
Analogues of drugs for maintaining pregnancy
After in vitro fertilization, it is necessary to replenish the lack of natural estradiol. To do this, use the drug Proginova. It contains synthetic estradiol (estradiol valeriate), which allows the fetus to attach itself to the uterine wall.
The dosage form of the drug is a dragee for oral administration. The scheme of application is developed individually by the fertility specialist in charge of the pregnancy, taking into account all contraindications and research results.
Proginova is not prescribed in the following cases:
- with endometriosis;
- if there are malignant neoplasms of the liver;
- with diabetes of any type;
- with increased blood clotting ability;
- if the pregnant woman is overweight.
It is impossible to cancel the drug on your own, as this can have consequences up to termination of pregnancy. The dosage is reduced gradually, the individual course is calculated by the doctor.
Another progesterone drug is Crinon. It is available in the form of suppositories or gel. Most often, candles are prescribed, their use is easier. The drug can be used once a day, which is more convenient for patients than multiple doses.
Conclusion
The prescription of the drug must be carried out by a doctor. It is unacceptable to self-administer, replace the drug with a similar one, change the regimen or completely cancel it. Self-medication in this case threatens to disrupt the long-awaited pregnancy.
Video: Pregnancy management after IVF



