Inflammatory process of the mucous membrane treatment. What causes inflammation of the cervix. How is the diagnosis carried out?
Vaginitis is one of the most common reasons women visiting a gynecologist. This disease affects the entire vaginal mucosa.
Gynecological diseases are not rare. According to statistics, every third woman has some kind of disease related to the pelvic organs. The most common ailment is vaginitis. It is characterized by inflammation of the vaginal mucosa.
Ulcerative colitis is an inflammation of the large and small intestine that usually involves only the superficial mucosa. Ignition spreads far upward in different ways. If the inflammation is limited to the rectum, it is called proctitis. If the inflammation spreads to the entire large intestine, the so-called complete picture of the disease occurs.
Ulcerative colitis is thought to be caused by several factors, with one suggesting a multifactorial event. It should be taken for granted that environmental influences play a role, since ulcerative colitis is increasing in incidence and is much more common in high-tech countries of the world than in all other regions. Role psychological factors is controversial.
Causes of vaginitis
- Most main reason The reason why the disease occurs is the presence of diseases such as chlamydia, gonorrhea, trichomoniasis and the like.
- Senile vaginal atrophy.
- Poor personal hygiene.
- Insertion of foreign objects into the vagina.
- Use of antibiotics.
- Promiscuous sex life.
- Incorrect douching.
- Prolapse of the vaginal walls.
- Poor quality abortion.
- Decreased immunity.
- Allergic reaction.
- Gaping of the genital slit. It may arise due to the personal physiological characteristics of a woman.
- Beginning of sexual activity.
All of these reasons contribute to the fact that a favorable environment is created in the vagina for the proliferation of pathogenic bacteria. In addition to the diseases listed above, vaginitis can occur due to E. coli.
The overwhelming consensus is that although mental stress can trigger an existing condition, it is not the cause of inflammatory bowel disease. Numerous studies show that, due to individual location, the immune responses of the body's immune system are directed against components in the intestines.
From twin and family studies, it is known that hereditary factors play an important role in chronic inflammatory bowel disease. For example, identical twins have a 40% higher risk of infection. For siblings and children of those affected, the risk is only 2-5%.
Symptoms of the disease
Vaginitis can be acute or chronic. In the chronic stage, the disease occurs with mild symptoms that appear before or after menstruation.
Symptoms of acute vaginitis
- A woman may notice that there is more discharge. They changed color and acquired an unpleasant odor.
- The discharge has become cloudy in color, viscous, and quite often becomes stretchy.
- If the inflammatory process has already begun, then pus is observed in the discharge.
- With trichomonas vaginitis, the discharge takes on a fishy smell and becomes foamy. When vaginitis occurs due to a fungal infection, the discharge is white and cheesy in nature.
- There is itching in the groin area.
- The labia are red and often increase in size.
- Sexual contact brings pain.
- Body temperature may rise, especially if the vaginal walls are severely affected.
- Sometimes unpleasant pain occurs during urination. Pain may also occur in the lumbar region.
- There is also a burning sensation.
Symptoms of the chronic form
In addition to general symptoms such as loss of power, fatigue, loss of appetite and sometimes fever, the main symptoms of the disease are directly related to the intestines. The most common bleeding occurs during bowel movements. The stool is usually dark and mixed with mucus. Leakage of blood without stool may also occur. The frequency of bowel movements can range from 10 to 20 times a day. In addition, pain is felt in the colon, in the middle of the lower abdomen or in the Kreuzbeingegend. Patients often experience pain before or immediately after passing stool.
- Copious discharge.
- Painful menstruation.
- The appearance of pronounced symptoms after hypothermia.
If the patient complains of any symptoms, she is sent for diagnostic procedures.
How is the diagnosis done?
First of all, the patient is listened to and then examined in a gynecological chair. An experienced doctor will determine the presence of vaginitis immediately after examination, but an accurate diagnosis requires testing.
Because iron is always lost in the blood, the bone marrow does not have the iron it needs to make new blood. The result is so-called iron deficiency anemia. Symptoms of the disease occur in batches. An acute episode can last up to two months and occur several times a year. In between there are phases that are almost asymptomatic. The general condition worsens, fatigue and pallor indicate anemia and protein deficiency. Later, poor vision, painful skin changes on lower limbs and joint inflammation.
The gynecologist may send the patient to the treatment room or take a vaginal smear during the examination. The laboratory conducts a detailed examination of the samples and determines what kind of vaginitis the patient has. In rare cases, a woman may be prescribed additional tests, such as blood and urine tests. When the results of the study are ready, the doctor prescribes treatment.
But spontaneous healing is possible in rare cases. Although no specific form of diet is recommended for chronic inflammatory bowel disease, it is natural to do everything on the nutritional side to not irritate the intestines and to provide the body with all the necessary nutrients sufficient.
The most important information for a doctor is the symptoms and their impact on daily life. Therefore, it is worth doing a weekly protocol with information about the frequency of bowel movements, the condition of the stool such as hard, soft or watery, blood on the stool, abdominal pain, general well-being, weight and body temperature.
How are vaginitis treated?
If the patient experiences purulent discharge, the doctor prescribes anti-inflammatory therapy. It consists of taking antibiotics or using them in the form of ointments. The woman is also prescribed douching. Antiseptic solutions and astringent decoctions are used for it. If treatment is ineffective and there is a tendency to relapse, the woman is prescribed estrogen hormones.
These observations have been made in outpatient and hospitalized patients with allergies, and their findings deserve attention and sensitivity on the part of the treating physician. Ultimately, urinary tract infections increase. Allergy of the upper respiratory tract and esophagogastroduodenitis. Sinusitis and soft stools with mucus sometimes stink. Acute respiratory viral infections and soft stools, and sometimes diarrhea. Coincidence of tonsillitis with pain in the right iliac fossa, simulating appendicitis or diffuse abdominal pain.
Gastroesophageal reflux and recurrent respiratory tract infections. The emergence of a geographic tongue with acute viral respiratory infections. Urinary infection and vulvovaginitis associated with allergic enteropathy. There is some overlap in some of these manifestations reported in the medical literature.

It is worth noting that special attention is paid to the treatment of vaginitis in pregnant women. The doctor, first of all, tries to remove the inflammatory processes, and only then treat the immediate disease. The difficulty of treatment lies in the fact that a pregnant woman is contraindicated to take antibiotics and drugs that suppress bacteria, which caused vaginitis.
Clinical association of tonsillitis and right iliac fossa pain simulating acute appendicitis 6 The important thing to be attentive to the global adherence of the mucous membranes in a given patient is that their diagnostic and therapeutic approach should be holistic and individualized.
Lack of response to the treatment of pathology associated with a certain mucous membrane in allergic diseases, we see this every day in our medical practice, when we ignore the adherence to another mucous membrane that is simultaneously compromised, for example.
In order to prevent the disease, doctors advise their patients to monitor personal hygiene, maintain a measured sex life and visit a gynecologist at least 4 times a year.
Inflammatory diseases of the external genital organs in women consistently occupy a leading position in the structure of visits to the gynecologist. About 60% of patients of various ages complain of itching, burning and vaginal discharge of various types. Moreover, previously the bulk of these patients were women of mature and elderly age, but now there is a steady increase in young girls in the structure of morbidity.
Unresponsive asthmatic patient with uncontrolled rhinitis. Persistent asthma due to undiagnosed bacterial sinusitis. Otherwise it would be incompetent. For example, an otolaryngologist could not treat a runny nose unless he was treating intestinal disorders for the first time; gynecologists or urologists could not treat the high percentage of vulvovaginitis and urinary infections without first treating respiratory allergies and intestinal disorders; Likewise, a pulmonologist will not diagnose gastritis unless he intentionally finds them; as well as other specialties related to allergic disease.
This is due to the almost universal distribution of risk factors, the combination of which inevitably develops an inflammatory process in the vagina - vaginitis. Moreover, a particular problem is caused by primarily chronic forms of the disease, characterized by a poor clinical picture. Since the manifestations do not bother the woman much, she is not in too much of a hurry to treat the existing vaginal inflammation.
This clinical approach is the pathophysiological dependence of the mucous allergic disease, completely reconsidering the treatment to this day is established by traditional medicine, each of the mucous membranes of the immune information is not processed slightly differently, however, there is an immunological cross of information between them. For example, a food allergen can simultaneously cause symptoms in the digestive and respiratory systems. 7.
Food allergies can coincide with allergies to aeroallergens up to 70% 8, which increases the likelihood of cross-reactions of food with aeroallergens. These findings implicate the intestine as an important source of antigen generation and should therefore be considered when treating the allergic patient, regardless of where the allergic disease manifests.
The disease itself is not as dangerous as the long-term consequences of its uncontrolled course. Regardless of the pathogen, the inflammatory process tends to ascend. That is, pathological changes, while risk factors remain, can contact the internal genital organs. But their defeat is much more serious in terms of course and prognosis, especially for women of reproductive age.
The experience of our research group is that after the patient does a proper diet, healthy bowel hygiene and control environment, allergies disappear in a high percentage. Another mistake in medical practice is to consider these symptoms as a disease. In fact, these are symptoms or signs of allergic diseases; the correct diagnosis for an allergic patient should be: an allergic disease with manifestations of esophagitis, gastritis, rhinitis, asthma, vulvovaginitis, etc. to consider an organ compromised in isolation from the rest of the body, one must ignore that the mucous membranes share immunological information and that attachment to it can have consequences, on the other.
Reasons
Considering the mechanisms of development of the disease, the leading place in its development is occupied by acquired risk factors. Moreover, the main ones among them are those that create conditions for reducing the protective forces of the mucous membrane:
- In first place is widespread hormonal contraception. Although it was previously indicated that its cyclic use only has a beneficial effect on the reproductive system, now the opinion has changed dramatically. The selection of a drug should only be carried out strictly taking into account all indications and contraindications.
- This is followed by a steady increase in functional and organic gynecological diseases leading to disruption menstrual cycle. Changes in hormonal regulation at any level inevitably affect the condition of the vaginal mucosa and microflora.
- A gradual increase in endocrine pathology in the female population - diabetes mellitus, obesity, thyroid dysfunction.
- Triggering factors include changes in sexual behavior, violation of personal hygiene rules, and a decrease in the protective forces of the immune system. These include frequent changes of sexual partners, regular use of barrier contraception, irrational washing and douching, and existing foci of chronic infection.
For ease of diagnosis and treatment of vaginal inflammation, the causes of its occurrence were divided into two groups - those caused by opportunistic or special microbes.
Finally, another aspect that should be reconsidered as research is carried out is that ascending urinary tract infection and vulvovaginitis may be associated with suffering of the mucous membrane close, as in the case of constipation or allergic enteropathy, or at a distance, as in the case of allergic rhinosinusitis. There are already studies implicating allergic disease as a cause of vulvovaginitis, 9 including an association with dust mite allergy. In my opinion this problem is very common and medical literature does not yet describe it as such.
Specific
This group of pathogens mostly consists of microorganisms transmitted primarily through sexual contact. In fact, the inflammation of the vagina caused by them is a sexually transmitted disease. Therefore, this variant of the disease develops quite acutely and requires immediate treatment:
Let this study motivate research to clarify the prevalence of this syndrome in allergic disease, establish a new definition of it and explore the relationship of the latter with other processes of mucosal suffering, such as adult gastroesophageal reflux, vesicoureteral reflux, adult interstitial cystitis, constipation and endometriosis.
The scientific basis that explains the pathophysiology of mucosal inflammation syndrome in allergic disease is based on a new concept in modern psychoneuroendocrine immunology, which we hope to develop in the next volume. Recent publications on allergies have focused on rhinitis and asthma as manifestations of the same process. Confirmation by other investigators of simultaneous mucosal involvement in an allergic patient would help validate the new definition of allergic disease and therefore facilitate a new therapeutic approach.
- The most common is trichomonas vaginitis, a specific lesion caused by protozoa. Its development is accompanied by itching, discomfort and copious foamy vaginal discharge.
- Next in frequency are inflammatory processes caused by intracellular pathogens - chlamydia or mycoplasma. Their peculiarity is a hidden course; moderate symptoms (burning, scanty mucous discharge) are rarely observed.
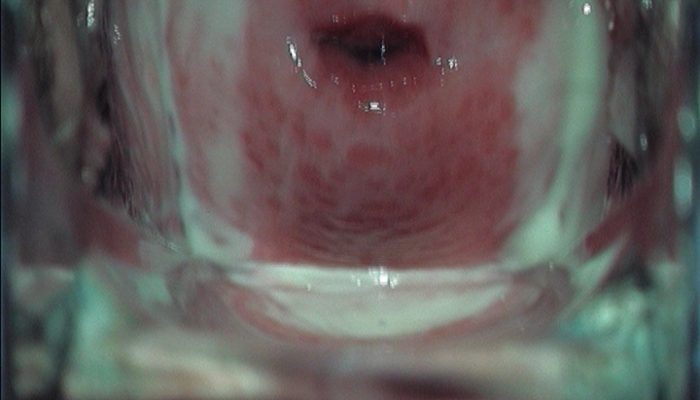
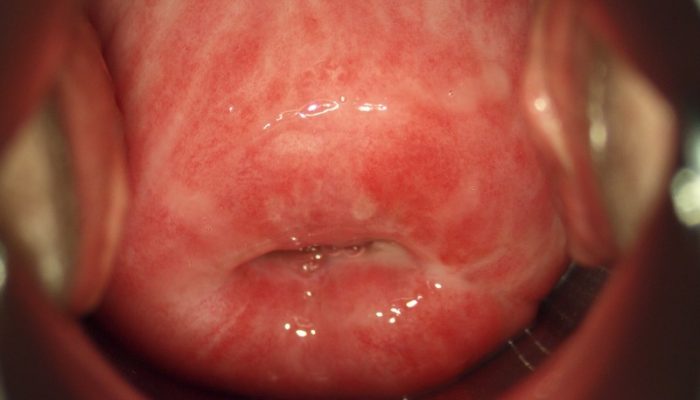
- Inflammation of the vaginal mucosa caused by gonococci is quite rare; damage to the cervix is more typical. But with its development, a bright clinic is observed - a strong burning sensation and the formation of copious purulent discharge.
- Candidal vaginitis is now also classified as a sexually transmitted disease. Fungi of the genus Candida normally live on the vaginal mucosa, but under favorable conditions they can multiply uncontrollably, causing itching and cheesy discharge.
If any specific vaginitis is suspected, the attending physician must confirm it using special diagnostic methods.
10-year prognosis for allergic rhinitis in children. Asthma and wheezing in the first six years of life. El-Serag, Mark Gilger, Mark Kuebeler, Linda Rabeneck. Extrasophageal associations of gastroesophageal reflux disease in children without neurological defects. Lessin, Mark, Ailawadi, Manesh and sausages. Prevalence of sensitization to food allergens in Swedish adults. Allergy: European Journal of Allergy and Clinical Immunology. Routine evaluation and treatment of vulvovaginitis. Clinical obstetrics and gynecology.
Allergic vulvovaginitis caused by house mites: a case report. Vulvodynia is a complex pathology and difficult to treat. It is defined as chronic vulvar pain that can be generalized or localized. They usually consult several times and different doctors before arriving at a diagnosis. There are no specific tests, so the clinic and physical examination are the main tools. All of these pathologies that explain this chronic vulvar pain should be excluded. Its etiology is multifactorial, including changes at the nociceptor level, changes in innervation, and the presence of inflammatory factors.
Non-specific
In this case, inflammation of the vagina is caused by microorganisms that belong to the opportunistic inhabitants of the skin. Two factors lead to the development of the disease - a decrease in local immune activity and a decrease in the number of lactobacilli on the mucous membrane. This leads to the colonization of the “empty” space by microbes, and the formation of an inflammatory response to their introduction:
However, we cannot ignore psychosexual aspects that may modulate or trigger vulvar pain by finding an altered substrate at the level of these tissues. Based on these aspects, today there are various treatments that are effective if we use them associated and in stages as they become stronger among them.
A large number of gynecologists do not know this diagnosis. For this reason, women consult several times and with different doctors to establish a diagnosis. There are no special tests for diagnosis. Search through clinical and physical examination is the primary tool for this diagnosis. Should be excluded various pathologies which could explain the presence of chronic vulver pain. IOS of multifactorial etiology Undoubtedly, changes in the number of nociceptor involvement changes and additions to innervation and the presence of inflammatory factors, which may be the starting point of ESTA pathology, as it seeks to explain the neuropathic theory.
- The first variant of the development of the disease is more common in postmenopausal women, and is called bacterial vaginosis. It is characterized by the replacement of the normal vaginal microflora (lactic acid bacteria) with specific rods - gardnerella. In this case, inflammatory changes are mild, and the main complaint is moderate discharge with an unpleasant fishy odor.
- The second option is more typical for women of young and reproductive age. Inflammation of the vagina occurs against the background of a decrease in protective forces, which leads to the aggressive displacement of lactobacilli by more aggressive flora - staphylococci, streptococci, and intestinal microbes. In this case, obvious signs of damage are observed - redness and swelling of the mucous membrane, burning and itching, copious mucous or purulent discharge.
Approximate knowledge of the differences between individual forms of vaginitis allows you to begin effective therapy even before receiving laboratory diagnostic results.
Treatment

Help for patients with acute or chronic forms must necessarily consist of two parts. Compliance with this principle will not only eliminate existing symptoms, but also prevent relapse of the disease in the future:
- For vaginal inflammation of any origin, treatment should begin with general measures. They should include stimulation of the immune defenses - elimination of chronic foci of infection, normalization of diet and rest. For specific vaginitis, unprotected sexual intercourse must be excluded and systemic antimicrobial therapy is carried out.
- General treatment must be effectively supplemented with local treatment in order to create conditions for mechanical removal of the pathogen from the mucous membrane. For this purpose, local forms of drugs are used - vaginal tablets, suppositories and ointments, as well as douching with antiseptics.
Compliance with the principles and timing of treatment will eliminate the present manifestations, and correction of risk factors will prevent their possible relapse.
Specific

If any of the listed infections in this group is suspected, a course of general antimicrobial therapy must be prescribed. Isolated implementation of only local procedures will not only not lead to recovery, but will also create conditions for the chronic course of the disease:
- Treatment of trichomonas vaginitis is carried out with the help of antibiotics - derivatives of 5-nitroimidazole - Metronidazole, Ornidazole, Tinidazole. They are prescribed internally, as well as locally - using ointment applications or suppositories.
- Therapy for chlamydial and mycoplasma inflammation of the vagina is carried out using macrolides - antibiotics that act on intracellular pathogens. The drugs Azithromycin, Clarithromycin or Josamycin are prescribed. In addition to them, local baths or douches with antiseptics are used - Betadine, Chlorhexidine or Miramistin.
- Gonorrheal vaginitis is treated with combination therapy - a combination of Ceftriaxone with Azithromycin or Doxycyline is prescribed. It is also complemented by mandatory local procedures.
- Treatment of candidiasis is carried out only with the help of antifungal drugs, initially applied only locally - Clotrimazole, Ketoconazole. If the result is insufficient, the doctor prescribes another course of systemic therapy.
After clinical recovery, vaginal smears are re-examined, confirming the complete destruction of the pathogen.
Non-specific

If the inflammation of the vagina is caused by opportunistic flora, then the treatment should not be so intense, but must be comprehensive. The goal of assistance is not only to eliminate the pathogen, but also to maximize fast recovery normal vaginal microflora:
- First of all, risk factors are identified - chronic infections, endocrine diseases, lifestyle features. A consultation is held regarding their further elimination, and the necessary prescriptions are given.
- General and local antibacterial therapy is currently not widely used. Prescription of drugs from this group is carried out only for specific indications. Only products with a combined effect are used - Terzhinan, Polygynax, Neo-Penotran, a combination of Metronidazole and Clindamycin.
- Baths and douches with antiseptics (Chlorhexidine, Betadine, Miramistin) are prescribed for a period of no more than 3 days. This time is enough to destroy the bulk of pathogens, without affecting the remaining lactobacilli.
- Immediately after completion of local antimicrobial therapy, eubiotics are prescribed - agents that restore normal microflora. These include the drugs Vagilak, Bifidumbacterin, Lactobacterin, Biovestin.
- For atrophic changes in the mucous membrane, local forms of estrogens are additionally used - Ovestin.
But still, the basis of treatment for nonspecific variants of the disease is modification of the woman’s health status and lifestyle. Only active identification and treatment of concomitant diseases and conditions will avoid the return of unpleasant symptoms.